Indian Health Service: Opportunities Exist to Improve Clinician Screening Adherence and Oversight
Fast Facts
The Indian Health Service provides health care to American Indians and Alaska Natives. To ensure that its patients are receiving quality care, IHS screens the clinicians it employs—e.g., doctors and nurse practitioners—to verify their professional qualifications.
However, federal IHS facilities didn't always fully follow the requirements for verifying these qualifications. This is partly because IHS's guidance on how to do so is spread out across multiple, and sometimes conflicting, documents.
We recommended, among other things, that IHS develop a single, authoritative document that includes its screening requirements and how to meet them.
Highlights
What GAO Found
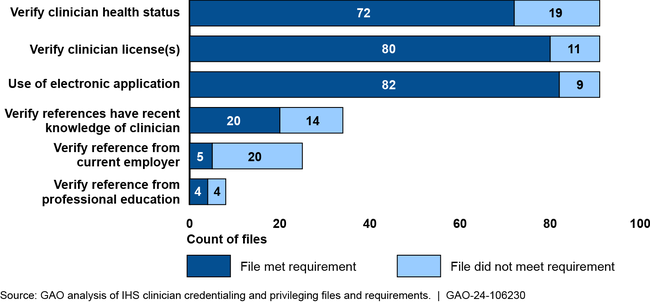
To provide patients with the highest level of care at its federally operated facilities, the Indian Health Service (IHS) reviews and verifies professional qualifications of clinicians through a process known as credentialing and privileging. GAO found that existing IHS oversight methods did not ensure adherence to all of IHS's credentialing and privileging requirements. GAO's review of a random nongeneralizable sample of 91 clinician files found that IHS generally met some of the requirements reviewed. However, IHS did not meet six of the requirements in 10 percent or more of the applicable files GAO reviewed. (Some of these requirements only apply to clinicians new to IHS.)
Indian Health Service (IHS) Adherence to Selected Credentialing and Privileging Requirements
This lack of adherence was due to IHS not having a single, comprehensive source of its credentialing and privileging requirements and limited monitoring by headquarters. Currently, IHS requirements are spread across multiple, sometimes conflicting, documents, making it challenging for officials to know of and meet them. Further, existing IHS oversight is concentrated at the local level and does not routinely include headquarters' reviews of clinicians' files for adherence with IHS requirements. IHS officials said they plan to improve guidance and oversight, but plans are in initial stages and have not yet been implemented. Until it ensures clinicians are appropriately screened, IHS risks hiring or retaining clinicians with performance, health, or other issues, potentially affecting the quality of care provided to patients and putting them at risk.
The 24 IHS clinicians from federally operated facilities who GAO interviewed reported performing a range of tasks they considered to be administrative, including entering data in IHS's electronic health record (EHR) system and communicating about patient care. They varied in the time they estimated spending on administrative tasks; 11 clinicians said they spent 20 percent or less of their time, while 13 said they spent from 21 to 50 percent of their time on such tasks. Clinicians who previously worked in non-IHS facilities generally reported spending less time performing administrative tasks at those facilities than at their IHS facilities. They attributed the difference to non-IHS facilities having a superior EHR, fewer training requirements, or more administrative support.
Why GAO Did This Study
IHS provides health care services to 2.8 million American Indians and Alaska Natives, including through a system of federally operated facilities. Clinician competence and excessive time spent on administrative tasks are factors that can affect the quality of care that clinicians provide.
GAO was asked to review IHS clinician screening and the performance of administrative tasks. This report examines IHS oversight of credentialing and privileging. It also describes administrative tasks performed by IHS clinicians at federally operated facilities.
GAO reviewed IHS policies and other documents, including the most recently available credentialing and privileging file for a random nongeneralizable sample of 91 clinicians. GAO also interviewed officials from IHS headquarters and nine geographic areas, as well as a random nongeneralizable sample of 24 clinicians who were working at an IHS federally operated facility.
Recommendations
GAO is making three recommendations, including that IHS should (1) develop a single, authoritative source outlining procedures to meet its credentialing and privileging requirements and (2) implement regular headquarters' monitoring of adherence to credentialing and privileging requirements. The agency concurred with all three recommendations.
Recommendations for Executive Action
| Agency Affected | Recommendation | Status |
|---|---|---|
| Indian Health Service | The Director of IHS should develop a single, authoritative source that clearly defines the procedures and steps to meet national credentialing and privileging requirements. (Recommendation 1) |
IHS agreed with GAO's recommendation. On October 30, 2024, IHS published a Medical Staff Credentialing and Privileging Standard Operating Procedure Manual. This manual defines the procedures and steps to meet IHS's national credentialing and privileging requirements in a single, authoritative source.
|
| Indian Health Service | The Director of IHS should develop and implement a process to review and update the single, authoritative source of credentialing and privileging requirements, once developed, to ensure that it is updated in a timely manner to reflect any changes in those requirements. (Recommendation 2) |
IHS agreed with GAO's recommendation and has begun taking steps to implement it. IHS updated its Indian Health Manual to include a requirement for its Medical Staff Credentialing and Privileging Standard Operating Procedure Manual (SOP) to be reviewed and updated biennially. According to IHS, the goal of that review is to ensure that the SOP is current and contains appropriate and adequate policy information and procedural guidelines for IHS staff members to effectively perform their duties and responsibilities. In addition, the SOP notes that staff can provide IHS's Office of Quality with suggestions and edits to the SOP and other credentialing and privileging documents. However, neither the Indian Health Manual nor the SOP clearly delineate how the Office of Quality will maintain and make timely updates to the SOP during the intervening periods between the biennial reviews. To close the recommendation as implemented, IHS needs to show that it has conducted biennial reviews and updated the manual, as necessary, in a timely manner, including in the intervening periods between the biennial reviews.
|
| Indian Health Service | The Director of IHS should implement regular monitoring of areas' and facilities' adherence to IHS's credentialing and privileging requirements by headquarters officials. Such monitoring could include, headquarter officials conducting audits or reviews of a sample of credentialing and privileging files, and regular reviews of audits conducted by area offices and facilities. (Recommendation 3) |
IHS agreed with GAO's recommendation. IHS's Indian Health Manual delineates staff responsibilities for oversight and monitoring of credentialing and privileging compliance. In addition, its Medical Staff Credentialing and Privileging Standard Operating Procedure Manual (SOP) establishes standards for compliance and includes audit tools that can be used for conducting audits of providers' credentialing files. IHS told us that headquarters officials will perform manual audits on a random sample of providers' credentialing files and report compliance rates in a quarterly report to leadership. However, neither the Indian Health Manual nor or the SOP specify (1) the frequency of audits that will be conducted by headquarters officials or (2) the information that would be reported to IHS leadership. To close the recommendation as implemented, IHS needs to show that headquarters officials have actually implemented regular monitoring of areas' and facilities' adherence to IHS's credentialing and privileging requirements, such as evidence that the IHS Office of Quality has conducted regular audits of a random sample of providers' credentialing files.
|